Improving Penta Vaccine Uptake Through Clinical Communication in Cameroon

In 2024, the Bali Health District in Cameroon faced alarmingly low Penta vaccine uptake among children under 5 years. Penta vaccination is crucial for preventing five deadly diseases (diphtheria, tetanus, pertussis or whooping cough, hepatitis B and Haemophilus influenzae type b). Every missed Penta dose left a child vulnerable to these potentially life-threatening illnesses. Despite the importance of this vaccine, gaps in clinical communication left many caregivers misinformed, hesitant or unaware of the need for timely vaccination. To tackle this challenge, Effective Basic Services (eBASE) Africa, with support from JBI, implemented a structured, evidence-based approach to improve vaccine communication. Using JBI methodology––an internationally recognised framework for evidence implementation––the team identified best practices and worked collaboratively with local health providers to close communication gaps and strengthen vaccine uptake in the community.
Background
Bali Health District is a rural region in Cameroon with over 30,000 residents, many of whom rely on subsistence farming and face barriers to healthcare access. Vaccination drop-out rates were high, driven by communication failures, limited reminders and lack of caregiver engagement. In fact, some mothers often walked long distances to Infant Welfare Clinics, only to leave more confused about follow-up dates or side-effects than when they arrived. Healthcare providers often lacked structured tools and current guidelines for interacting with mothers during Infant Welfare Clinics . Low uptake of vaccines such as Penta contributes to the persistence of preventable diseases, increasing the risk of outbreaks, hospitalisation and even child mortality. According to district health reports from 2023, the Penta vaccine drop-out rate from Penta 1 to Penta 3 was approximately 30%, far exceeding the acceptable threshold of less than 10%. This alarming gap highlights the urgent need for effective, evidence-based communication strategies to improve caregiver engagement and reduce preventable illnesses.
The primary issue addressed by this project was the low uptake of the pentavalent vaccine among children under 5 years in the Bali Health District, Cameroon. This challenge had been observed over time through both routine immunisation data and feedback from community health workers and caregivers. Many mothers were unaware of the full benefits of vaccination, had misconceptions about side-effects and often missed appointments due to lack of reminders or clarity on follow-up schedules. According to district health records, the drop-out rate from Penta 1 to Penta 3 was 30% in 2023, meaning nearly one in three children who started the vaccine series did not complete it. One nurse reflected, “We just told the mothers to come back in a month—we didn’t explain what the vaccines were for or why it was important to return.” Health workers lacked training in effective communication and did not consistently provide evidence-based information. There were also no standardised communication protocols or educational tools available across facilities.
Implementing evidence
Using JBI's PACES and GRiP frameworks , a multidisciplinary team was assembled to lead the project. The team included the District Medical Officer, data managers, nurses and midwives responsible for vaccination at the Infant Welfare Clinics and four trained research assistants from eBASE Africa, a local NGO. JBI’s PACES (Practical Application of Clinical Evidence System) tool was used to assess current communication practices and identify gaps in provider-caregiver interactions. JBI’s GRiP (Getting Research into Practice) approach guided the development of context-specific strategies to overcome these barriers.
Strategies included developing a clinical communication protocol, conducting staff training sessions, distributing posters, sending SMS reminders and engaging community health workers. The clinical communication protocol was developed based on WHO recommendations and evidence from similar interventions in Sub-Saharan Africa. It outlined clear talking points for explaining each vaccine dose, managing caregiver concerns about side-effects and scheduling follow-up visits. The protocol was pilot tested with health workers at two clinics, who provided feedback on language, cultural relevance and usability before final rollout.

Figure 1: Penta Vaccine Campaign Poster
The broader set of communication materials, including posters and counselling aids, were co-designed by the research team in collaboration with nurses, community health workers and district staff. Caregivers were consulted through informal group discussions to review drafts and suggest culturally appropriate adjustments. An example of one of the posters is shown in Figure 1. It featured colourful illustrations and simple language in English and Pidgin English, highlighting the five diseases covered by the Penta vaccine and the importance of completing all three doses.
Community health workers were engaged through face-to-face planning sessions and brief training workshops. They played a key role in refining the communication strategy and later supported home visits to follow up with caregivers who missed clinic appointments.
More than 400 SMS reminders were sent to caregivers ahead of follow-up visits, while a separate set of over 400 evidence-based messages was shared with providers to reinforce best practices. Visual coaching tools were used during IWC sessions to engage caregivers. These tools included laminated flip charts with simple images explaining the five diseases prevented by the Penta vaccine, the vaccination schedule and common side-effects. Health workers used them as visual aids during one-on-one counselling to simplify communication, especially for caregivers with low literacy levels.
“We realised it wasn’t just about giving vaccines — it was about how we communicated them,” said Ngem Bede, project lead. This realisation prompted the team to approach communication as a clinical intervention.
Demonstrating impact with evidence
“Now we don’t just vaccinate, we talk to the mothers, we explain,” shared a nurse from Bossa Integrated Health Center. Another community health worker noted, “With the list of dropouts, I can find children who missed their vaccines and follow up.” Nurses also reported greater confidence in communicating with caregivers, especially around managing concerns about vaccine safety. This was captured during feedback sessions held after training, where providers shared their experiences using the communication protocol. Caregivers were observed asking more follow-up questions during IWC sessions, particularly about side-effects and when to return for the next dose, which was recorded in daily logs.
A follow-up audit revealed dramatic improvements in nine out of ten criteria (see Figure 2). Compliance rates rose across the board, with indicators such as education on adverse events increasing from 23% to 71% and provision of reminder messages rising from 15% to 64%. Drop-out lists were shared through churches and njangi (rotating savings) groups and community health workers reported improved capacity to track and follow up with caregivers. These platforms were chosen because they are trusted, community spaces where caregivers regularly gather. Sharing information through churches and njangi groups helped ensure that messages reached caregivers in a familiar, supportive environment. These results demonstrated the power of communication in transforming public health outcomes
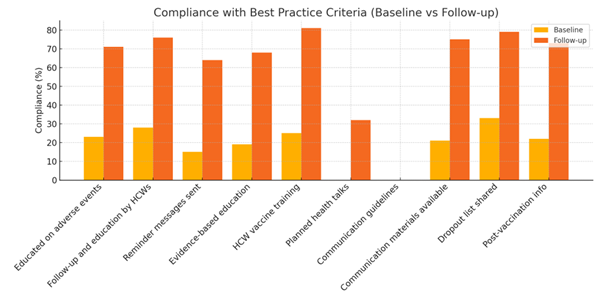
Figure 2: Summary of baseline and follow-up audit results
Table 1 below summarises baseline and follow-up compliance with the ten best practice criteria tracked throughout the project. Improvements were seen in 9 out of 10 areas, with particularly notable increases in health worker training, use of reminder messages and caregiver education.
Table 1: Baseline and follow-up compliance with best practice criteria
| Audit Criterion | Baseline Compliance (%) | Follow-up Compliance (%) |
|---|---|---|
| Educated on adverse events | 23 | 71 |
| Follow-up and education of healthcare workers | 28 | 76 |
| Reminder messages sent | 15 | 64 |
| Evidence-based education | 19 | 68 |
| Healthcare worker vaccine training | 25 | 81 |
| Planned health talks | 0 | 32 |
| Communication guidelines | 0 | 0 |
| Communication materials available | 21 | 75 |
| Drop-out list shared | 33 | 79 |
| Post-vaccination info | 22 | 73 |
Challenges and lessons learned
Resource constraints, outdated norms and cultural resistance were key barriers. Some healthcare workers continued to use old practices, believing that writing dates on vaccination cards was sufficient. Community health workers lacked transportation and tools for active case tracking. Others were hesitant to adopt the new communication protocol, unsure whether caregivers would understand or respond to it.
The project addressed each challenge step by step. For outdated communication habits, hands-on training sessions helped health workers practice the new approach, using real-life scenarios. One nurse explained, “At first, I thought just giving the date was enough. But now I see how much more the mothers understand when I explain the why.” We needed about 400 posters to reach the over 200 communities in Bali and Batibo Health Districts. This was a challenge because we were not able to fund the printing of these posters. This greatly limited our reach.
For community health workers without resources, support was provided in the form of printed drop-out lists, transport to pay for bikes in some hard-to-reach areas and mobile recharge vouchers to follow up on missed appointments. Caregivers also noticed the difference. “Before, they would just write a date on the card. Now they explain everything. I don’t miss appointments anymore,” said one caregiver. The project overcame these challenges through stakeholder engagement, cost-effective technology (e.g., SMS), and use of WhatsApp for continuous knowledge sharing. WhatsApp groups were created for community health workers and health workers across participating facilities. These groups were used to share reminders, answer questions, post weekly tips on communication and troubleshoot challenges in real time. District supervisors also used the platform to provide encouragement and rapid feedback. Participation remained active throughout the project, with most community health workers checking in weekly.

Sustainability and next steps
The project laid the foundation for sustainable practice change by embedding audit feedback into monthly district review meetings and engaging leadership at all levels. Moving forward, the Bamenda-3 Health District is leading efforts to scale up the intervention, with technical support from eBASE Africa and oversight from the Cameroon Ministry of Public Health. Refresher training is scheduled to be held quarterly. District health authorities have also committed to including communication quality indicators in routine supervision checklists to reinforce good practices. Over the next 12 months, the communication protocol and supporting tools will be rolled out to three additional health districts, starting with Batibo and Bamenda. “This project has shown us that improving communication is not just a soft skill—it’s a system priority … we are committed to making this part of how we do things, district-wide,” said the District Chief of Bureau Health. These steps are supported by continued collaboration with regional partners to ensure that effective communication becomes a lasting part of routine immunisation practices.
Conclusion
Improving communication led to a measurable increase in vaccine uptake and caregiver satisfaction in Bali Health District. This project shows how targeted evidence implementation can bridge the gap between intention and impact, making clinical communication a powerful tool in the fight against vaccine-preventable diseases. As a result, more children in the district are now fully protected against life-threatening illnesses such as diphtheria, tetanus and hepatitis B. Caregivers feel more informed, confident and supported—and health workers are better equipped to provide not just services but understanding. At its core, this project is a story of trust rebuilt, lives protected, and communities strengthened through better communication.
Key takeaways
- Clinical communication is essential for improving vaccine uptake and trust.
- Evidence-based strategies can drive change, even in low-resource settings.
- Stakeholder collaboration is key to overcoming systemic barriers.
- SMS, visual tools and community engagement are effective, scalable interventions.
References
World health Organization. Immunization coverage [internet]. WHO; 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
Beatrice A, Frascella F, Oradini-Alacreu C, Balzarini P, Signorelli LA. Effectiveness of email-based reminders to increase vaccine uptake: a systematic review. Vaccine. 2019:433-443.
JBI. Products and services [internet]. JBI; 2025. Available: https://jbi.global/products.
Okwen P, Ngem B. Reducing the burden of malaria in children under five years of age in Cameroon. Effective Basic services Africa. Bamenda; 2016.
To link to this article - DOI: https://doi.org/10.46658/JBIIM-25-08
Authors
Ngem Bede, Lontum Alvin and Akah Thelma Eni
JBI Effective Basic Services Africa Cameroon