Building Evidence-Based Ayurvedic Diabetes Care in Nepal

Bridging the gap between evidence and practice for Ayurvedic diabetes care in Nepal
Type 2 diabetes mellitus is a growing public health challenge across South Asia, including Nepal, where health systems are under increasing pressure from chronic diseases. Many people seek care from Ayurveda, a long-established traditional healthcare system widely used in both urban and rural communities. Ayurvedic practitioners play a key role in both public and private care and are often the first point of contact for patients.
Despite its widespread use in diabetes management, there are concerns about variation in clinical practice and suboptimal care among Ayurvedic practitioners. These concerns primarily arise from the routine use of formulations that are untested, ineffective, or potentially unsafe. This highlights a clear gap between routine clinical practice and the available scientific evidence. Currently, there is no clinical guideline for diabetes management in this setting, and Ayurvedic practitioners lack access to synthesised evidence to support day-to-day clinical decision-making.
Given the established role of Ayurveda in Nepal, there is a clear need to work collaboratively with the system to strengthen it and enhance its potential through evidence-informed practice.

Synthesising Evidence on Ayurvedic Medicines for Diabetes Management
The work began with a systematic review protocol developed using JBI methodology to evaluate the effectiveness and safety of Ayurvedic medicines for diabetes management. The review applied rigorous evidence synthesis methods, including assessment of the certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, which considers risk of bias, inconsistency, indirectness, imprecision, and publication bias.
The completed systematic review and meta-analysis synthesised evidence from 199 randomised controlled trials involving more than 21,000 participants and 98 Ayurvedic medicines. The findings showed promising improvements in blood glucose control while also highlighting important weaknesses in study quality and the need for stronger future research. Beyond synthesising available evidence, the review created a foundation for translating research into clinical practice within a traditional healthcare system where no clinical guideline previously existed.

Developing an Evidence-Based Clinical Guideline
Building on the systematic review findings, the multidisciplinary team developed a clinical guideline to support Ayurvedic practitioners in managing diabetes. This was an important step for Ayurvedic diabetes care. The development process combined evidence synthesis with expert consultation and stakeholder engagement to ensure recommendations were clinically practical, contextually appropriate, and supported more consistent decision-making.
The clinical guideline provided structured recommendations on patient management, lifestyle advice, and treatment approaches grounded in systematically synthesised evidence. Additional general recommendations, including lifestyle advice, were adapted from Western medicine clinical guidelines. Through these outputs, the work demonstrated how evidence synthesis can extend beyond academic publication to directly support healthcare improvement.
Assessing the Feasibility of Clinical Guideline Implementation in Nepal
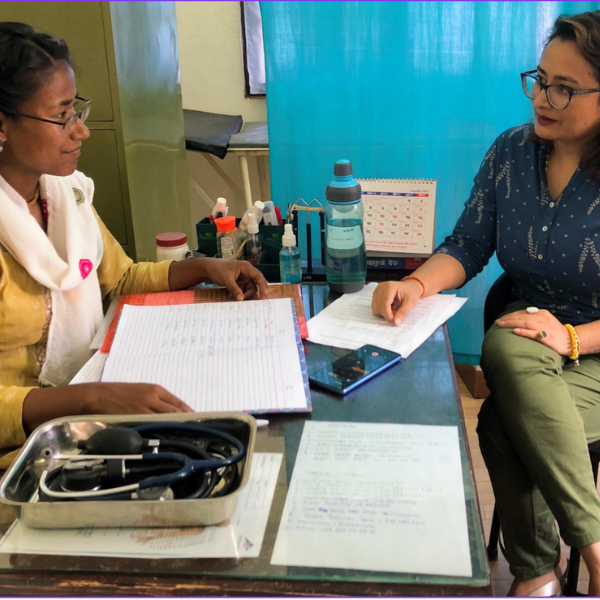
To assess whether the clinical guideline could be implemented in routine practice, the multidisciplinary team conducted a feasibility cluster randomised controlled trial in Nepal, following a published protocol, involving public and private Ayurveda centres within and outside the Kathmandu Valley. Implementation strategies included regular guideline training sessions for Ayurvedic practitioners, a structured guideline-based template for clinical case notes, and provision of the guideline-recommended Ayurvedic medicine at clinics for free prescription.

A total of 121 people with diabetes were recruited (60 in the clinical guideline-based arm and 61 in the usual care arm), with 84% followed up to six months (51 per group). Median practitioner adherence to the clinical guideline indicated partial to adequate adherence. The median number of guideline-recommended medicines not consumed and days without consumption were zero. No serious adverse events were reported. Preliminary findings suggested potential beneficial effects on blood glucose levels and health-related quality of life, although these were not statistically significant.
Alongside the feasibility trial, a qualitative study explored the experiences and perspectives of participating Ayurvedic practitioners and patients through interviews. The findings showed that the evidence-based clinical guideline approach, together with implementation strategies, was well received and perceived as more beneficial than usual clinical practice, which participants described as inconsistent and of suboptimal quality.
Ayurvedic practitioners reported improved consistency in prescribing and clearer clinical decision-making. As one noted, ‘Fixed standard drugs would ensure uniformity; currently, one Ayurvedic doctor might prescribe differently than another.’
Others highlighted improved confidence and safety in practice, stating, ‘We didn’t have to prescribe untested medicine, which reassured patients’, and ‘Clearer treatment protocols would simplify practice.’
The clinical guideline was also described as improving structure and reducing variation, with Ayurvedic practitioners noting, ‘Sticking to the guideline ensured consistency across our work’, and ‘The clear guideline minimized errors and deviations.’
Several reported changes in routine care, including more systematic counselling and referrals: ‘I advise patients on medication, diet, exercise, and lifestyle modifications according to the guideline’, and ‘Following the guideline, I referred a patient because his HbA1c level increased.’
Ayurvedic practitioners also described broader improvements in care quality and communication, noting that ‘Guideline-based management is more structured than usual care, which is often vague’, and ‘The guideline made it easier to explain things to patients and build trust.’ Many emphasised the value of structured, evidence-informed practice, stating, ‘Evidence-based clinical practice is crucial’, and ‘Following the guideline benefits both patients and doctors with clear instructions. It improves patient health and encourages follow-ups.’
Patients similarly reported positive experiences, describing improvements in their condition and reassurance from guideline-based treatment, noting, ‘When my sugar levels were high, we were worried, but this medicine brought them under control’, and ‘The medicine, along with monthly advice and follow-ups, has improved my health.’ Patients also suggested expanding this clinical guideline approach to other chronic diseases, with one stating, ‘If this kind of Ayurvedic treatment could be expanded to other diseases, it would be beneficial.’
The Role of JBI Methodology and Training
JBI methodology played a central role in the evidence synthesis phase of the project. The evidence synthesis leads were trained in JBI systematic review methods and served as trainers, supported by other team members trained in JBI systematic review methodology. The systematic review followed JBI guidance for effective reviews and used the JBI critical appraisal tool for randomised controlled trials to assess methodological quality.
These rigorous and transparent methods generated a reliable evidence base that informed both the clinical guideline and subsequent implementation research. This work demonstrated how robust evidence synthesis methodology can support healthcare improvement not only in Western medicine but also in traditional healthcare systems such as Ayurveda.
Collaboration Across Disciplines and Countries
Funded by the United Kingdom’s Foreign, Commonwealth and Development Office (FCDO), Medical Research Council (MRC), National Institute for Health and Care Research (NIHR), and Wellcome Trust, a major strength of the initiative was its collaborative and multidisciplinary approach. The work was grounded in equity, diversity, and inclusion, with shared ownership of decisions across partners in the Global North and Global South in Nepal, India, and the United Kingdom.
Furthermore, the project brought together researchers, Ayurvedic and Western medicine practitioners, policymakers and decision-makers, and community representatives. This collaboration helped ensure methodological rigor while remaining sensitive to local healthcare realities and the traditional healthcare system. It also strengthened research capacity in evidence synthesis, implementation science, and evidence-informed healthcare across participating settings.
Sustainability and Future Directions
Several participating Ayurvedic practitioners reported that the clinical guideline became an integral part of their routine clinical practice after the project, and they continued delivering guideline-based care. The clinical guideline provides a framework that can continue evolving as stronger evidence becomes available. Ayurvedic practitioners and patients also suggested expanding this approach to other chronic diseases.
The initiative established an important foundation for future work on evidence-informed Ayurveda and chronic disease management and generated practical lessons to inform future large-scale implementation of evidence-informed Ayurvedic care. More broadly, it demonstrated that traditional healthcare systems can engage meaningfully with evidence-based healthcare approaches.
Conclusion
Using JBI evidence synthesis methodology, the multidisciplinary team conducted a systematic review of evidence on Ayurvedic medicines for type 2 diabetes, developed an evidence-based clinical guideline for Ayurvedic practitioners, and assessed the feasibility of the guideline’s implementation in Nepal. The findings indicated that evidence-informed Ayurvedic diabetes care was both feasible and acceptable in practice.
Overall, the initiative demonstrated how JBI-informed evidence synthesis can support meaningful healthcare improvement within traditional healthcare systems, without losing cultural identity or clinical relevance, by translating fragmented evidence into practical clinical guidance. The work also highlighted that evidence alone is not sufficient to improve practice. Effective change requires a strong contextual understanding, collaboration, and sustained engagement with key stakeholders.
References:
Chattopadhyay, K., Dhimal, M., Karki, S., Regmi, P., Bista, B., Biswas, T. K., Heinrich, M., Panniyammakal, J., Tandon, N., Leonardi-Bee, J., Kinra, S., Greenfield, S. M., Lewis, S. A., Upadhyay, V., & Gyanwali, P. (2022). A clinical guideline-based management of type 2 diabetes by Ayurvedic practitioners in Nepal: A feasibility cluster randomized controlled trial protocol. Medicine, 101(47), e31452. https://doi.org/10.1097/MD.0000000000031452
Chattopadhyay, K., Kapoor, N., Heinrich, M., Mitra, A., Mittal, M., Lewis, S. A., Greenfield, S. M., Mukherjee, S., Pischel, I., Jeemon, P., Tandon, N., Kinra, S., Biswas, T. K., & Leonardi-Bee, J. (2023). Development process of a clinical guideline to manage type 2 diabetes in adults by Ayurvedic practitioners. Frontiers in Medicine, 10, 1043715. https://doi.org/10.3389/fmed.2023.1043715
Chattopadhyay, K., Karki, S., Wang, H., Regmi, P., Gyanwali, P., Upadhyay, V., Heinrich, M., Bista, B., Tandon, N., Kinra, S., Greenfield, S. M., Biswas, T. K., Jeemon, P., Leonardi-Bee, J., Lewis, S. A., & Dhimal, M. (2026). Diabetes management by Ayurvedic practitioners using a clinical guideline versus usual practice: A feasibility cluster randomized trial in Nepal. Journal of Diabetes Research, 2026, e2602864. https://doi.org/10.1155/jdr/2602864
Chattopadhyay, K., Panniyammakal, J., Biswas, T. K., Heinrich, M., Lewis, S. A., Greenfield, S. M., Tandon, N., Kinra, S., & Leonardi-Bee, J. (2020). Effectiveness and safety of Ayurvedic medicines in type 2 diabetes mellitus management: A systematic review protocol. JBI Evidence Synthesis, 18(11), 2380–2389. https://doi.org/10.11124/JBISRIR-D-19-00350
Chattopadhyay, K., Rana, N., Karki, S., Regmi, P., Gyanwali, P., Upadhyay, V., Bista, B., Tandon, N., Kinra, S., Biswas, T. K., Leonardi-Bee, J., Heinrich, M., Panniyammakal, J., Lewis, S. A., Greenfield, S. M., & Dhimal, M. (2026). Diabetes management using a clinical guideline versus usual practice: A feasibility trial-based qualitative study among Ayurvedic practitioners and patients in Nepal. Therapeutic Advances in Endocrinology and Metabolism, 17. https://doi.org/10.1177/20420188261417088
Chattopadhyay, K., Wang, H., Kaur, J., Nalbant, G., Almaqhawi, A., Kundakci, B., Panniyammakal, J., Heinrich, M., Lewis, S. A., Greenfield, S. M., Tandon, N., Biswas, T. K., Kinra, S., & Leonardi-Bee, J. (2022). Effectiveness and safety of Ayurvedic medicines in type 2 diabetes mellitus management: A systematic review and meta-analysis. Frontiers in Pharmacology, 13, 821810. https://doi.org/10.3389/fphar.2022.821810
Authors
Dr Kaushik Chattopadhyay, Prof Jo Leonardi-Bee