
Physical Activity and Endogenous Pain Modulation in Older Adults
Mapping an Emerging and Conceptually Complex Evidence Base
Pain is common in older adulthood and is associated with substantial impacts on quality of life. With ageing, recovery from injury or illness often slows, potentially increasing vulnerability to persistent pain. Against this background, physical activity is frequently discussed as a non-pharmacological approach to pain management, particularly in light of concerns about polypharmacy in later life. Despite this interest, the mechanisms through which physical activity may influence pain in older adults remain incompletely understood.
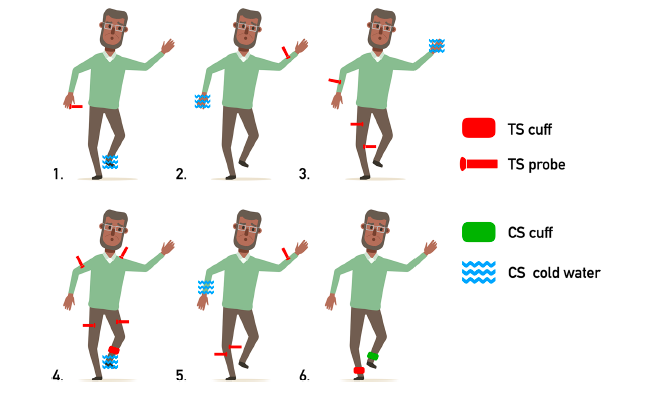
One mechanism that has received increasing attention is endogenous pain modulation, which refers to processes by which the central nervous system regulates pain perception. A widely used method for examining this capacity is conditioned pain modulation. In this paradigm, pain is first assessed using a test stimulus and then reassessed following the application of a second, painful conditioning stimulus. In many individuals, exposure to the conditioning stimulus results in a reduction in perceived pain from the test stimulus, consistent with inhibitory pain control. In older adults and in people with chronic pain, however, this inhibitory response is often attenuated and may, in some cases, be replaced by increased pain sensitivity.
A new scoping review aimed to map existing research on the relationship between physical activity and endogenous pain modulation in older adults, with a particular focus on studies assessing pain modulation using conditioned pain modulation. Rather than evaluating intervention effectiveness, the review sought to describe how this relationship has been studied and to identify areas of conceptual and methodological inconsistency.
Across the included literature, physical activity was conceptualised in diverse ways. Some studies examined acute exercise exposures, such as brief isometric or aerobic tasks, while others focused on longer-term exercise programmes or habitual physical activity measured objectively. This variation reflects the breadth of physical activity as a construct, but it also highlights a lack of consensus regarding which dimensions of activity are most relevant for studying pain modulation in later life.
Evidence linking physical activity to conditioned pain modulation was mixed. Some studies reported associations between higher levels of physical activity and more effective pain inhibition, with indications that activity of at least moderate intensity may be particularly relevant. At the same time, substantial variability was observed across studies and individuals. This variability was especially evident in populations with knee osteoarthritis, where exercise-related exposures were associated with reduced pain sensitivity in some participants but increased pain in others.
The review also underscores the importance of distinguishing between related but distinct concepts. Exercise-induced hypoalgesia refers to short-term reductions in pain sensitivity that occur during or shortly after exercise, whereas conditioned pain modulation is a psychophysical paradigm used to assess the efficiency of inhibitory pain pathways. Although both are linked to endogenous pain control, they capture different processes. Across studies, these concepts were not always clearly delineated, complicating interpretation and comparison of findings.
Many studies modified exercise protocols for older participants, for example by adjusting intensity or load, but these adaptations were often minimally described and rarely accounted for the wide variation in health status, functional capacity, and pain sensitivity observed with ageing. In addition, conditioned pain modulation was assessed using diverse protocols, further limiting comparability across studies.
The scoping review brings structure to a heterogeneous body of evidence. It suggests that physical activity may be related to endogenous pain modulation in older adults, but that this relationship is variable and context-dependent. Key questions remain regarding how pain modulation capacity should be characterised in later life, how different forms and intensities of physical activity engage these mechanisms, and how individual differences shape outcomes. By mapping what has been studied and how, the review clarifies both the current state of the field and the areas where further conceptual and methodological work is needed.
The scoping review, Physical activity and endogenous pain modulation in older people, is available in the current issue of JBI Evidence Synthesis.