
Reducing etomidate-induced myoclonus
The most effective pharmacologic agent
A recently published umbrella review provides an important analysis of the relative effectiveness of various pharmacologic agents to reduce the incidence and severity of etomidate-induced myoclonus. The review determines the most effective pharmacologic agent, among both opioids and non-opioids, to lower the incidence and severity of myoclonus associated with etomidate administration for the induction of general anaesthesia.
Adverse effects of etomidate
Etomidate is a commonly used sedative-hypnotic in anaesthesia practice, used as an induction agent for general anaesthesia to facilitate tracheal intubation. It is frequently used as an alternative to propofol and barbiturates due to its favourable haemodynamic profile in patients with cardiovascular instability.
However, etomidate has been shown to induce adrenal suppression, which has negative implications for patient mortality in the postoperative period. Etomidate also carries a high risk of postoperative nausea and vomiting, and causes myoclonus in up to 80% of patients.

Impact of myoclonus
Myoclonus, similar to convulsive seizures, can lead to damage to muscle fibres, myalgias, elevated serum potassium levels, and an increased risk of gastric contents aspiration.
Myoclonus induces a hypermetabolic state, increasing oxygen consumption, which can be detrimental for patients with pre-existing hypertension, aneurysms, and coronary artery disease. Myoclonus will further increase intraocular pressures and may result in vitreous prolapse for trauma patients or those undergoing ophthalmic surgery.
Reducing the impact of myoclonus
Methods to reduce the impact of myoclonus in patients given etomidate have been proposed. These include pre-treatment with opioids (such as butorphanol, dezocine, remifentanil), lidocaine, dexmedetomidine, and benzodiazepines.
With so many prophylactic options available, each with their own set of potential side effects and varying degrees of effectiveness, anaesthesia providers would benefit from a determination of which pharmacologic treatment offers the most reliable prevention of myoclonus when etomidate administration is necessary.
Conflicting evidence
Multiple randomised controlled trials, and systematic reviews and meta-analyses have been conducted to determine the most effective method of pre-treatment to prevent or reduce etomidate-induced myoclonus (including Wang et al Efficacy and Safety of Opioids for the Prevention of Etomidate-Induced Myoclonus: A Meta-Analysis; Zhou et al Effect of pretreatment with midazolam on etomidate-induced myoclonus: A meta-analysis; and Lang et al Pretreatment with lidocaine reduces both incidence and severity of etomidate-induced myoclonus: a meta-analysis of randomized controlled trials). However, conflicting evidence regarding the most effective pharmacologic agents for preventing or reducing etomidate-induced myoclonus has left anaesthesia providers without a definitive answer to the question: What is the most effective prophylactic treatment?
A review of systematic reviews
An umbrella review has just been published in JBI Evidence Synthesis on pharmacological interventions for reducing the incidence of myoclonus in patients receiving etomidate for induction of general anaesthesia.
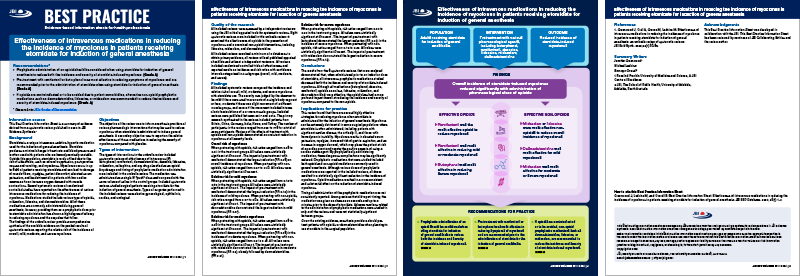
The umbrella review included eight systematic reviews (which included 48 randomised control trials) that examined intravenous pharmacologic agents used to reduce etomidate-induced myoclonus at the time of general anaesthesia induction, including butorphanol, dexmedetomidine, dezocine, lidocaine, midazolam, nalbuphine, and any drug classified as an opioid.
Most effective prophylactic medications to reduce myoclonus
All pharmacologic interventions identified in the umbrella review demonstrated a statistically significant reduction in the incidence of myoclonus when administered prophylactically ahead of an induction dose of etomidate.
The absolute risk reduction indicating the effectiveness of the prophylactic medications ranged from 47% to 81% for mild, 52% to 92% for moderate, and 61% to 96% for severe myoclonus.
Opioids demonstrated the most consistent and substantial effect on reducing the incidence and severity in myoclonus compared with non-opioids.
A JBI Best Practice Information Sheet accompanies the published umbrella review. It provides a summary of the review and best practice recommendations for anaesthesia providers.
The umbrella review is published in the January 2024 issue of JBI Evidence Synthesis:
Greenwood, Jennifer; Crull, Allison; Graves, Melissa; Ledvina, Michael
JBI Evidence Synthesis 22(1):p 66-89, January 2024. | DOI: 10.11124/JBIES-22-00390